An ambulatory surgical center (ASC) is a healthcare facility that focuses on providing same-day surgical care that includes diagnostic and preventative surgery. When looking at the ASC, it has transformed the outpatient surgical experience for millions of Americans by providing a more convenient surgical alternative. As much as 65% of all surgical cases performed take place in the outpatient ASC setting.
Perioperative pressure Injury risk in ASC
When considering same day surgery, it may appear a safer alternative to inpatient surgery; even though an estimated 1-6% of outpatient surgeries are associated with complications requiring a 30-day hospital admission. This statistic may be because of the more complex surgical cases performed at the ASC. While there are many advantages to having surgery at an ASC, perioperative pressure injury (PPI) risks do not change.
Research shows that PPI occurrences are still prevalent in the inpatient surgical setting (40.1%). This percentage may be related to the unique surgical environment and extrinsic risk factors. The extrinsic factors contributing to PPI among surgical patients include surgical type, patient positioning, duration of anesthesia, amount of blood loss and use of pressure‐relieving devices (gel pads, heel troughs, prone position gel pads, and gel axillary rolls).nsibility of all perioperative nurses to protect the patient in any area of care.

Extrinsic factors contribute to pressure injuries
Additional extrinsic factors include the use of thermoregulation devices (the forced air, conductive warming, and heating lamps), and special perioperative circumstances (body temperature above 37°C, diastolic blood pressure below 60 mmHg, and oxyhemoglobin saturation by pulse oximetry (SPO2) below 93%)¹. Many of the above extrinsic risk factors do not change based on the inpatient or outpatient surgical facility. Thus, it is imperative to institute pressure injury prevention measures within both acute care and ASC settings.
Identify pressure injury risk by using a validated risk assessment tool
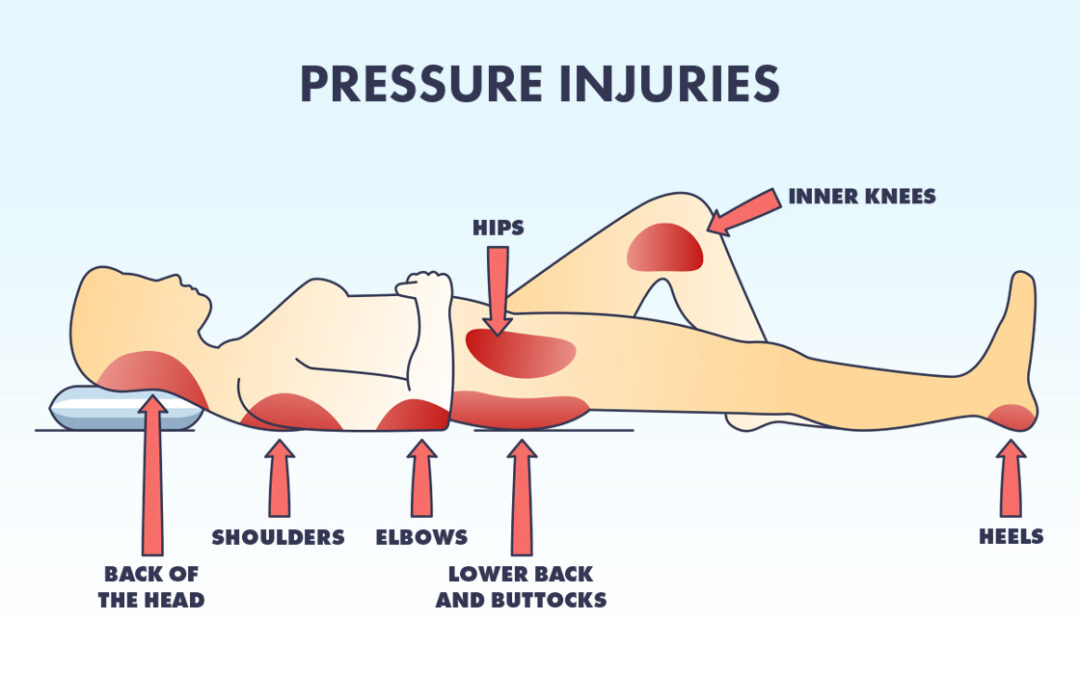
Identifying patients that are at risk for PPI by using a validated risk assessment tool is an important first step. Once the patient has been identified as high risk, evidence-based mitigation can be implemented. Pressure injury prevention (PIP) strategies can include using reactive gel surfaces for patient positioning which may be better than foam surfaces for preventing pressure injuries and are particularly relevant for patients undergoing surgery for several hours. Applying prophylactic materials (e.g., dressings, non-adherent devices designed to reduce PPI risk) to bony prominences (e.g., heels, sacrum) or other areas subjected to pressure, friction, and shear in patients identified as being at high risk for PPI (AORN Guidelines 2023). Offloading the supine patient’s heels (i.e., suspending the heels above the OR bed surface) increases perfusion and helps prevent PPI (AORN Guidelines 2023). Using intraoperative micro movements and offloading of bony prominence every 2.5-3 hours may also reduce the risk of PPI. For a complete list of pressure injury prevention strategies shown to decrease PPI risk, please refer to the AORN Guidelines: Prevention of Perioperative Pressure Injury.
Evidence-based interventions decrease pressure injury risk
As high-risk surgeries are transitioning to the ASC, perioperative pressure injuries are not only an inpatient problem. It is important to recognize that patient PPI risk is based on extrinsic risk factors and those risk factors do not change based on the environment of care. In addition, implementing evidence-based interventions decreases the PPI risk. It is the responsibility of all perioperative nurses to protect the patient in any area of care.
Resources
Weng, Pei‐Wei, and Wen‐Pei Chang. 2022. “Extrinsic Factors of Pressure Injuries in Patients during Surgery: A Frequency Matched Retrospective Study.” International Wound Journal 20 (6): 1934–42. https://doi.org/10.1111/iwj.14053.
B9027-000



